


When your erection fails, when your penis hurts or when you experience strange sensations in the pelvis, it’s rarely a coincidence. It’s often about very specific structures: the corpus luteum, blood vessels, nerves, connective tissue and the pelvic floor. I translate complex anatomy into something useful so you can understand what’s going on – and what I can do about it. My goal is for you to regain peace of mind and trust your penis again, whatever the situation.
Knowledge reduces uncertainty. When you understand why a symptom occurs, the next step becomes clear. I always bridge the gap between theory and practice, translating insights about penile anatomy into concrete actions that relieve pain, stabilize erection and increase sexual confidence.
The two upper cavernous bodies (corpora cavernosa) are the “engine” behind the erection. They fill with blood during sexual stimulation. For an erection to be hard, the blood must enter quickly and be effectively retained in the tissue (veno-occlusion). If the vessel wall or closure mechanism is weakened, the classic “semi-rigid” erection occurs. It can also cause pain or soreness in the bulging limbs.
The quality of tumor bodies depends on the ability of smooth muscles to relax and the health of blood vessels. Smoking, inactivity and metabolic issues can make the tissue less compliant. I assess whether the challenge is primarily ‘inflow’ (arteries), ‘outflow’ (veins) or muscle tone – because that determines what works.
The lower corpus spongiosum encloses the urethra and ends in the glans (head of the penis). It doesn’t get as hard as the corpora cavernosa – and that’s the point. Too much pressure here can squeeze the urethra. Pain in the glans or burning sensation can point to irritation of nerves or the mucous membrane in the urethra.
Sensitivity in glans varies naturally. If touch burns or stings, I work gently to calm nerves, optimize skincare and adjust friction during sex or masturbation (e.g. better lube and pace) to calm the irritation.
The tunica albuginea is the strong, fibrous “capsule” around the bulging organs. It distributes pressure during erection and keeps the blood inside. Thickenings or scar tissue (Peyronie’s plaque) here is at the heart of Peyronie’s disease and can cause curvature, pain, swelling, hourglass shape and loss of rigidity. On the outside is Buck’s fascia, which binds the structures together and protects the vessels and nerves.
When the tissue is repeatedly overloaded (e.g. by hard bending or microtrauma), the healing can form uneven scar tissue. I guide you in protecting the tissue until the irritation/inflammation is under control again, so the erection feels more stable and pain-free.
Signs of arterial weakness are often slow erections that do not reach full hardness. Signs of vein leakage are good starts that quickly slip away. I distinguish between these patterns because the treatment is different.
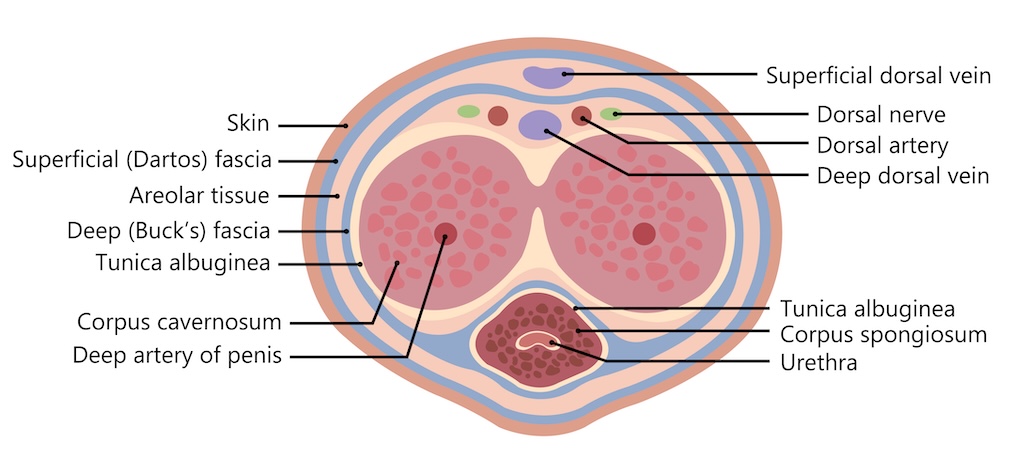
Sensation in the penis – and the ability to activate erection – is controlled by somatic and autonomic nerves, particularly via the pudendal and dorsal penile nerves. Irritation or pinching (e.g. from pelvic floor tension, cycling, scar tissue or lumbar nerve impingement) can cause sensory disturbances, pain, “electric shocks” or ejaculation problems.
I assess both the “conductivity” of the nerve and the tension of the surrounding tissue. Small changes in sitting position, saddle type or relief can significantly reduce irritation.
The foreskin protects the glans. A short frenulum breve or tight foreskin can cause pain, small tears and a “pulling” sensation during erection. It can also affect ejaculatory control and desire because the body instinctively holds back to avoid pain.
I assess mobility, skin elasticity and any scars. Often gentle stretching, good lubrication and customized stimulation help. If needed, I discuss how best to talk to your doctor about medical options.
The suspensory ligament anchors the penis to the pubic bone. It affects the angle of erection and stability. Soreness here can exacerbate pain during penetration or after sports.
Overstretching or sudden “kinking” can irritate the ligament.
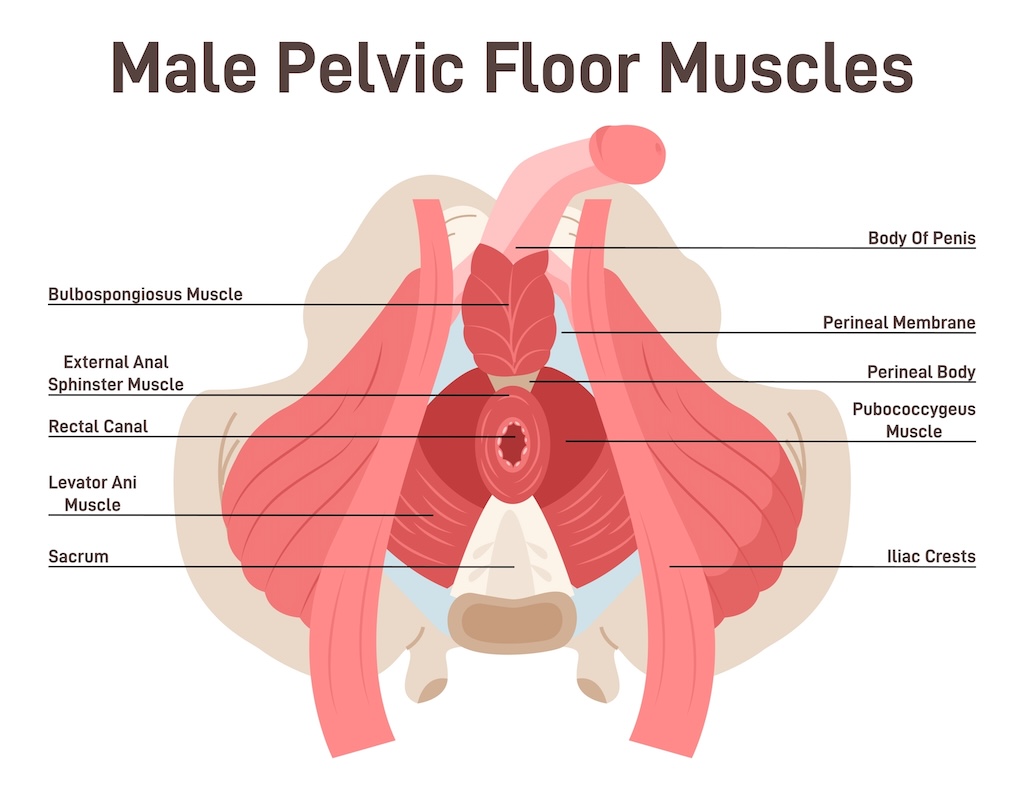
The urethra runs through the penis and is controlled by the pelvic floor muscles, among other things. The prostate lies just below the bladder and can affect urination and dribbling. An overactive or strained pelvic floor can cause pain, a “choppy” flow and an unpredictable erection.
I look at the interaction between the bladder, prostate and pelvic floor. Small adjustments in breathing and muscle coordination can often make urination more coherent and reduce dribbling, and shockwave and EMTT can help provide a better connection in the nervous system.
The parasympathetic nervous system (the body’s “rest and digest” system) promotes erection via the release of nitric oxide (NO). The sympathetic nervous system inhibits erection by releasing adrenaline and cortisol. Stress, pressure to perform, sleep deprivation and pain increase the sympathetic nervous system and can slow down erection even if you want to.
I use simple tools to shift the body towards calm: slow exhalations, safe touch, longer foreplay and a focus on pleasure rather than performance, as a complement to EMTT and shockwave therapy. It makes a noticeable difference in the signals to the penis.
NO causes vessels in the tumor bodies to dilate, allowing blood to flow in. The tunica albuginea ensures veno-occlusion – the mechanism that “locks” the blood in. Failure of one of these joints causes erectile dysfunction: e.g. poor endothelial function (due to diabetes, smoking, high blood pressure) or venous leakage. This is often seen in Peyronie’s disease
Exercise, smoke-free living and sleep boost NO levels and vascular function. Nicotine and chronic stress do the opposite. I’ll help you with realistic steps that are quickly noticeable in your recovery.
A well-functioning pelvic floor stabilizes the erection, helps keep blood in the penis and controls ejaculation. Overactivity causes pain, tingling, premature ejaculation or problems “slipping” into an erection. Under-activity can cause weak erection and after-dripping.
I teach you to feel the difference between “tightening” and “letting go” – and to connect the muscles with the breath. That coordination is often what’s been missing.
ED is often caused by a combination of decreased blood flow, vein leakage, nerve impingement and psychological factors such as performance anxiety. Signs of vein leakage are good initial erection, which quickly “oozes away”. Endothelial dysfunction is typically seen in lifestyle diseases. Both can be tested and targeted in a program. Shockwave has a proven effect in rebuilding the tissue structures in the penis
Morning erections are a good clue: if they are present, it indicates that the mechanics can function when the nervous system is calm. I use that knowledge to tailor the intervention – from vascular-focused treatment to nervous calm and pelvic floor.
Scar tissue in the tunica albuginea causes curvature, retractions, pain and erectile dysfunction. I assess the degree with ultrasound so I can target treatment: for example, focused shockwave for plaque and pain, EMTT for healing and tissue remodeling, and exercises and advice to protect the tissue in the active phase.
Peyronies typically occur in the connective tissue around the bulging bodies, where plaque or scar tissue can alter the elasticity of the penis. Read more about Peyronie’s plaque and penile scar tissue.
Gentle stretching and load management are key. I guide you on what is safe – and what should be avoided – so the curvature doesn’t worsen while the tissue is vulnerable.
Chronic pelvic pain (CPPS) often involves the pudendal nerve, pelvic floor trigger points and sensitized nervous system. It can feel like burning in the urethra, pain in the shaft of the penis, soreness in the bulge or stinging in the glans. A combination of neuromodulation, relaxation, breathing, graduated training and targeted pain management can help.
My focus is to lower the “alarm level” in the nervous system and create safe, gradual movement. You get concrete tools so that everyday life can once again accommodate activity without relapse.
A tight foreskin or short frenulum can cause pain, small tears, bleeding and inhibited desire. I assess motility, scar tissue and sensitivity and advise on gentle measures, skin care and realistic solutions. If necessary, I will guide you in talking to your own doctor about further investigation if surgery is being considered.
The goal is pain-free movement of the foreskin and free pleasure. Small adjustments in technique and pace often make a big difference from the very first week.
Post-void dribbling and light incontinence after urination can be about pelvic floor timing and urethra emptying. Targeted technique, breathing and muscle coordination often make a significant difference.
I teach you an effective emptying technique and the right sequence: first release, then empty, and finally a short activation to prevent leaks.
Nerve irritation from the pelvis or lower back, tight tissue along the shaft of the penis or scars can alter the sense of touch. Here I work with neuromodulation, gentle mobilization and sensory training to normalize the signals to the brain.
You’ll get simple home exercises that gradually “reset” your sense of touch so that touch feels pleasant again instead of painful or flat.
Both can be related to nerve sensitivity and pelvic floor patterns. With properly dosed exercise, breathing and sexology advice, you can regain control and confidence.
I use concrete methods such as pace control, pause-start and conscious breathing so you learn to regulate the pressure in your body – without losing your desire.
I use high-resolution ultrasound to assess tunica albuginea, possibly Peyronie’s plaque, vessel course and tissue quality. With Doppler, I can estimate blood flow and see signs of reduced supply.
The examination is respectful and at your pace. The images provide a clear visual overview, making it easier to choose the right treatment.
I test the pelvic floor’s strength, endurance and ability to tense-relax and examine the pudendal nerve with clinical neurodynamic tests. Many discover that this is the missing piece. We can also see your pelvic floor activity in real time, with ultrasound scanning, so you get a better sense of the area and what you can do.
You’ll get direct feedback along the way, so you’ll feel the difference between effective activation and unnecessary tension.
Sleep quality, stress levels, smoking, alcohol, medication and physical activity affect vessels, hormones and nerves. I go through it in a targeted way and make it easy to take action.
I prioritize 1-2 low-hanging fruits first so that you feel progress quickly and want to continue with more lifestyle changes.
If needed, I will guide you to talk to your doctor about relevant tests, such as testosterone, long-term blood sugar (HbA1c), lipids, metabolism and inflammation markers. This ensures that I don’t overlook medical causes that need to be treated in parallel.
I am happy to coordinate the process so that clinical training and medical treatment support each other.
Shockwave increases blood flow, stimulates tissue healing and can reduce pain. In Peyronie’s it can reduce pain and improve tissue quality; in ED it can strengthen microcirculation and endothelial function.
The treatment is non-invasive and takes place on the skin. I dose based on your findings and sensitivity, so it feels safe and effective.
EMTT affects cellular energy metabolism and healing processes. I use it for pain, scar tissue and nerve irritation – often in combination with shockwave for a stronger overall effect.
EMTT can be particularly useful when the tissue is “tired” and responds slowly to classic measures.
Targeted neuromodulation calms overactive nerves and normalizes signals to the pelvis and penis. It can reduce burning, tingling, “electric shocks” and improve erection control.
I supplement with home exercises that maintain the effect between treatments.
It’s rarely about “just squeezing”. I teach you how to regulate tension, coordinate with breath and gain strength in the right places. Many people get the best results from learning to let go before I build strength.
Timing makes all the difference: you need to be able to activate quickly when it counts – and release completely when your body needs to calm down.
Performance pressure, worries and bad experiences settle in the body. I work specifically with safety, timing, stimulation and communication – without taboos and with respect for your reality.
You can come alone or bring a partner. Shared understanding and calmness provide better conditions for pleasure.
Small, realistic changes in sleep, activity, weight, smoking and alcohol make a big difference to blood vessels and hormones. I’ll help you choose the 1-2 actions that will have the most impact now.
I always work with “least change with maximum impact” so you can maintain the results in your everyday life.
A slight curvature is normal. Sudden curvature, pain or retraction of the shaft points to Peyronie’s. I can clarify this with ultrasound and a clinical assessment – the earlier the better if you want to avoid many months of pain, low self-esteem and ultimately surgery.
Typical causes are reduced blood supply, venous leakage, pelvic floor disorders, nerve irritation, sleep and stress problems or side effects of medication. A targeted examination shows what applies to you – and thus the solution.
Yes, feeling cold and “flat” can be caused by microcirculation and nervous system tension levels. Shockwave, EMTT and pelvic floor and stress regulation can often improve it significantly.
No – not in itself. Pain, tearing or a feeling of “congestion” points to tight tissue, friction or bias. It can be adjusted with technique, lube, breaks and treatment of underlying causes.
Only if they are targeted. Many people already tense their pelvic floor too much. I often start with relaxation and coordination before strengthening. This results in a better erection and less pain.
Yes, you can. You can note if morning erections are present (signs of good physiology), if the erection lasts with stimulation, and if certain postures, breathing or stress affect. These observations help me to tailor your plan.
There is a lot of normal variation. What matters is function: the ability for painless erection, pleasure and control. If there is concern about size, I take it seriously – often it’s more about body image and comfort than anatomy.
Early signs such as shorter erections, slight curvature, new pain, burning or sensory disturbances are worth addressing. The sooner I help you take action, the easier it is to turn things around.
You don’t have to have “tried everything” to come – it’s my job to find the shortest path to recovery.
You walk away with an overview and a plan, no more questions.
I help men from all over Denmark – especially Copenhagen and Zealand – with targeted diagnostics and proven treatment of erectile dysfunction, Peyronie’s disease, chronic pelvic pain, incontinence and sexual performance problems. If you want a professional, concrete and respectful approach without taboos, book an appointment. Write or call and I’ll be happy to have the first, no-obligation chat about your symptoms, your anatomy – and your path back to safety and function.
If you are interested in hearing more about how I can help you, you are always welcome to contact me by phone 41 40 08 58 or email michael@msinsight.dk. I’ll get back to you quickly with a customized proposal so we can find the best way forward together.